Goa is abuzz with excitement as vintage bike and car owners, users, collectors and fans are decking […]
Old is Gold
October 4, 2016
ON May 12, 2026 The Lancet announced that Polycystic Ovary Syndrome (PCOS) would be renamed Polyendocrine Metabolic Ovarian Syndrome (PMOS). In this article we simplify the concept for you, explaining the scientific basis for the change, and emphasises the importance of holistic care for women’s health.
I AM sure most of you have heard of PCOS by now, though many may still have only a sketchy idea of what it really means. For years, millions of women were told they simply had a “cyst problem” and were advised to lose weight, take hormonal pills, or “wait until marriage” for their menstrual irregularities to settle.
However, science now tells us that Polycystic Ovary Syndrome (PCOS) is far more than just an ovarian disorder. In a landmark move led by global experts and endorsed by international medical bodies, the condition is now being renamed Polyendocrine Metabolic Ovarian Syndrome (PMOS) — a term that better reflects its true nature as a complex hormonal and metabolic disease.
The Science:
The change is not merely semantic. It marks a major shift in our understanding of one of the commonest endocrine disorders affecting women worldwide.
According to the World Health Organization (WHO), PMOS/PCOS affects approximately 8–13% of women of reproductive age, and nearly 70% remain undiagnosed globally. In India, the burden appears even higher in urban settings, with studies suggesting prevalence rates ranging from 10% to over 20% depending on diagnostic criteria and population studied.
Why Was the Name Changed?
The term “polycystic ovary syndrome” has always been problematic. Firstly, many women with the condition do not actually have ovarian cysts. Secondly, the “cysts” seen on ultrasound are not true cysts but immature follicles. Thirdly, the old name focused excessively on the ovaries while ignoring the underlying hormonal, metabolic, inflammatory and psychological disturbances.
The new term — Polyendocrine Metabolic Ovarian Syndrome — emphasises that the condition involves:
Multiple hormonal systems (polyendocrine)
Significant metabolic dysfunction including insulin resistance (metabolic)
Ovarian involvement, though not exclusively (ovarian syndrome)
This reclassification helps clinicians and patients understand that PMOS is not simply a fertility issue but a lifelong metabolic and endocrine disorder with systemic implications.
What Exactly Happens in PMOS?
At the heart of PMOS lies hormonal imbalance and insulin resistance.
In many patients, the body produces excess insulin because the cells do not respond effectively to it. This “insulin resistance” stimulates the ovaries to produce higher levels of androgens or male-type hormones such as testosterone. The result is irregular ovulation, menstrual disturbances, acne, unwanted facial hair growth, scalp hair thinning, and weight gain.
The condition is influenced by genetics, lifestyle, obesity, chronic inflammation, stress, sleep disturbances, and environmental factors. There is increasing evidence that PMOS begins during adolescence and may continue throughout reproductive life and beyond.
How Can One Recognise PMOS?
The presentation varies widely from person to person. Some women may be overweight, while others are lean. Some may have severe acne, while others present only with infertility.
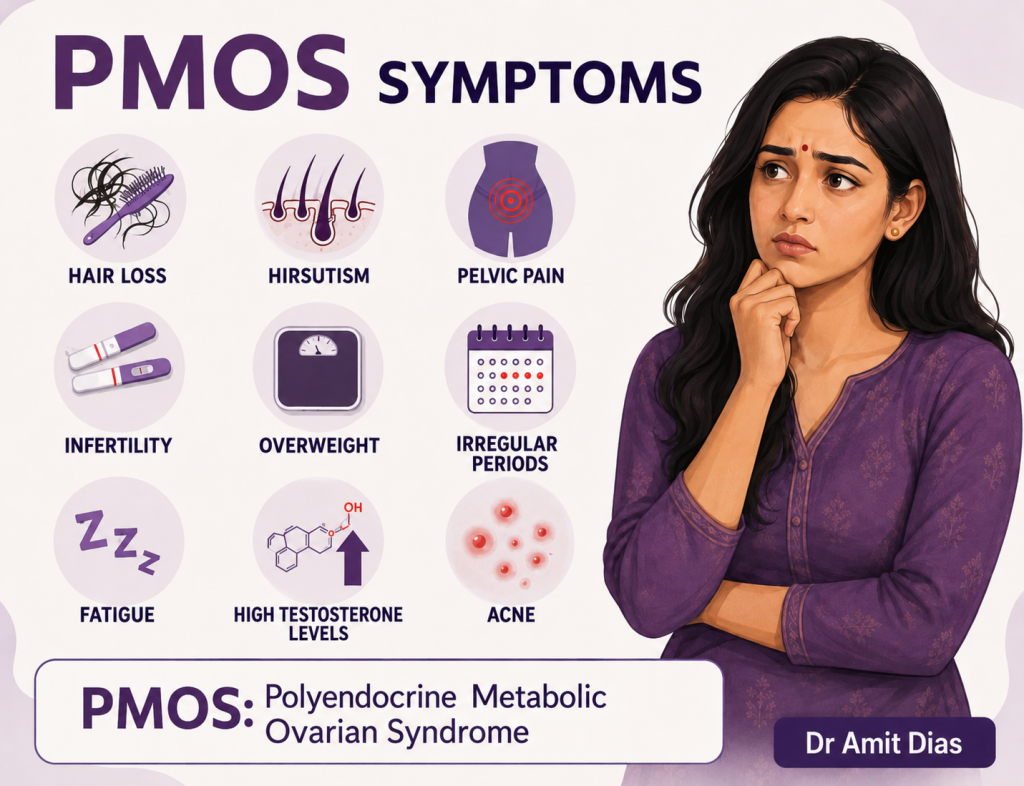
Common symptoms include:
— Irregular or absent menstrual periods
— Excess facial or body hair (hirsutism)
Acne or oily skin
— Weight gain, especially around the abdomen
— Difficulty conceiving
— Hair thinning or scalp hair loss
— Darkening of skin folds around the neck or armpits (acanthosis nigricans)
— Mood disorders, anxiety, or depression
— Fatigue and poor sleep
The diagnosis is generally based on the Rotterdam criteria, where two out of three features are present:
— Irregular ovulation or menstrual cycles
— Excess androgen activity (clinical or biochemical)
— Polycystic ovaries on ultrasound
PCOS vs PCOM: Understanding the Difference
A common source of confusion is the distinction between PCOS/PMOS and PCOM (Polycystic Ovarian Morphology).
PCOM refers only to the appearance of ovaries on ultrasound showing multiple small follicles. It is merely a radiological finding and can occur in healthy women, especially adolescents.
PMOS/PCOS, on the other hand, is a clinical syndrome involving hormonal and metabolic abnormalities along with symptoms.
Dispelling Common Myths
Myth 1: “Only overweight women get PMOS.”
False. Lean women can also develop PMOS due to hormonal and genetic factors.
Myth 2: “It is just a cosmetic problem.”
No. PMOS increases the risk of diabetes, hypertension, heart disease, infertility, and endometrial cancer.
Myth 3: “Pregnancy cures PMOS.”
Pregnancy may temporarily regulate cycles in some women, but the metabolic tendency persists.
Myth 4: “Irregular periods in teenagers are always normal.”
While some irregularity is expected after menarche, persistent abnormalities should not be ignored.
Myth 5: “Having cysts means surgery is needed.”
Most women do not require surgery. Treatment is primarily medical and lifestyle-based.
What Are the Long-Term Complications?
PMOS is increasingly recognised as a multisystem disorder.
Potential complications include:
— Type 2 diabetes mellitus
— Metabolic syndrome
— Obesity
— Fatty liver disease
— Infertility
— Miscarriage and pregnancy complications
— Hypertension
— Cardiovascular disease
— Sleep apnoea
— Anxiety and depression
—Endometrial hyperplasia and cancer
Women with PMOS often face psychological distress due to body image issues, infertility concerns, acne, and social stigma. Mental health screening is therefore an essential part of care.
The Treatment: A Holistic and Lifelong Approach
There is currently no permanent “cure” for PMOS, but the condition can be effectively managed.
Frequently Asked Questions
Here are answers to some of the frequently asked questions that we often get in our OPD.
Can PMOS be prevented?
While genetics cannot be changed, healthy lifestyle habits from adolescence may reduce severity and complications.
Is PMOS hereditary?
There is strong familial clustering, suggesting a genetic predisposition.
Can women with PMOS lead normal lives?
Absolutely. Early diagnosis and proper management allow most women to live healthy, productive lives.
Should every woman with irregular periods undergo testing?
Persistent menstrual irregularity, excessive hair growth, obesity, acne, or infertility should prompt medical evaluation.
A Public Health Priority
The renaming of PCOS to PMOS is more than a scientific update — it is a wake-up call.
Awareness among adolescents, parents, teachers, and healthcare providers is crucial. Early intervention can prevent long-term complications and improve quality of life.
The challenge today is not merely diagnosing PMOS, but ensuring that women are heard, validated, and treated holistically rather than symptomatically.
As science evolves, so must our language, our healthcare systems, and our attitudes toward women’s health.
 LETTER TO THE EDITOR FOR THE ISSUE DATED JULY 04, 2026
LETTER TO THE EDITOR FOR THE ISSUE DATED JULY 04, 2026 BATTLE WON BUT WAR REMAINS!
BATTLE WON BUT WAR REMAINS! BITCOIN FOR BEGINNERS! By Arvind Pinto
BITCOIN FOR BEGINNERS! By Arvind Pinto POLYMER NOTES, CLEANER CASH, NOT CURE-ALL!By Satish Singh
POLYMER NOTES, CLEANER CASH, NOT CURE-ALL!By Satish Singh WHEN IT COMES TO BIRTHDAY CAKES I STILL WANT TO ORDER `BOL SANS RIVAL’…By Tara Narayan
WHEN IT COMES TO BIRTHDAY CAKES I STILL WANT TO ORDER `BOL SANS RIVAL’…By Tara Narayan GOA’S 56-VILLAGE U-TURN EXPOSES DEEPER CRISIS OF TRUST! By Dr Olav & Deborah Albuquerque
GOA’S 56-VILLAGE U-TURN EXPOSES DEEPER CRISIS OF TRUST! By Dr Olav & Deborah Albuquerque DEV BOREM KORUM… FOR SHARING MY JOURNEY OF 43 YEARS IN GOA!
DEV BOREM KORUM… FOR SHARING MY JOURNEY OF 43 YEARS IN GOA! FROM SOMNATH’S PLUNDER TO ‘CHANDA CHORI’ IN AYODHYA!By Ram Puniyani
FROM SOMNATH’S PLUNDER TO ‘CHANDA CHORI’ IN AYODHYA!By Ram Puniyani A SPOONFUL OF CAUTION: THE HIDDEN STORY BEHIND THE COMMON COUGH SYRUP! By Dr Amit Dias, MD
A SPOONFUL OF CAUTION: THE HIDDEN STORY BEHIND THE COMMON COUGH SYRUP! By Dr Amit Dias, MD WEEKEND UPDATESLETTER TO THE EDITOR FOR THE ISSUE DATED JUNE 27, 2026
WEEKEND UPDATESLETTER TO THE EDITOR FOR THE ISSUE DATED JUNE 27, 2026 ROMI KONKANI IS FLOURISHING: Nagri Konkani is sinking!
ROMI KONKANI IS FLOURISHING: Nagri Konkani is sinking! SCALPEL & SCAM: HOW INDIA’S HEALTHCARE CRISIS IS FUELLED BY GREED, GRAFT & GOVERNMENT APATHY! By Uday Barad
SCALPEL & SCAM: HOW INDIA’S HEALTHCARE CRISIS IS FUELLED BY GREED, GRAFT & GOVERNMENT APATHY! By Uday Barad INDIA’S GIG ECONOMY: GOA’S FLEXIBLE FUTURE OR FRAGILE REALITY? By Arvind Pinto
INDIA’S GIG ECONOMY: GOA’S FLEXIBLE FUTURE OR FRAGILE REALITY? By Arvind Pinto COME THE MONSOON SEASON AND EVERYONE WANTS TO FEAST ON FRYUMS!By Tara Narayan
COME THE MONSOON SEASON AND EVERYONE WANTS TO FEAST ON FRYUMS!By Tara Narayan
Goa is abuzz with excitement as vintage bike and car owners, users, collectors and fans are decking […]