Goa is abuzz with excitement as vintage bike and car owners, users, collectors and fans are decking […]
Old is Gold
October 4, 2016
WHEN news of ebola disease outbreaks emerged from Africa, many people wondered whether the disease could reach India. In an age of global travel, infectious diseases can cross continents within hours. While ebola remains primarily confined to parts of Africa, the lessons learned from past outbreaks remind us that preparedness is not optional —it is essential.
The good news is that India has invested considerably in surveillance systems, laboratory capacity, infection prevention measures, and emergency response planning. We recently had a successful mock drill at the Goa Medical College monitored by the central government, to test the system in case we have a person with ebola. Yet preparedness is not merely the responsibility of governments and hospitals. An informed public is equally important and this article is an attempt to help raise awareness and not cause panic.
“Outbreaks do not respect borders. Preparedness is our strongest vaccine against fear.”
What is Ebola?
EBOLA Virus Disease (EVD) is a severe and often fatal illness caused by viruses belonging to the genus Ebolavirus. First identified in 1976 near the Ebola river in what is now the Democratic Republic of Congo, the disease quickly gained attention because of its high fatality rate and dramatic outbreaks.
Ebola is not a new disease. Scientists believe it originates from animal reservoirs, particularly fruit bats, which are considered the most likely natural hosts. The virus occasionally spills over from infected animals to humans, leading to outbreaks that can then spread through human-to-human transmission.
There are several species of Ebola virus, including Zaire, Sudan, Bundibugyo, Taï Forest, Reston, and Bombali viruses. The Zaire species has been responsible for the deadliest outbreaks, including the devastating West African epidemic between 2014 and 2016.
Why Does Ebola Keep Appearing in Africa?
A COMMON question is why ebola outbreaks predominantly occur in Africa. The answer lies in a combination of ecological, social, and healthcare factors.
The tropical forests of Central and West Africa provide an ideal habitat for fruit bats, which are believed to carry the virus without becoming ill. Human activities such as hunting, handling bushmeat, deforestation, mining, and encroachment into wildlife habitats increase opportunities for contact between infected animals and humans.
Once a spillover event occurs, several factors can facilitate transmission:
• Limited access to healthcare in remote regions.
• Delayed diagnosis due to overlap with diseases such as malaria and typhoid.
• Traditional burial practices involving direct contact with the deceased.
• Shortages of trained healthcare workers and infection control resources.
• Community mistrust and misinformation during outbreaks.
Importantly, ebola is not an “African disease.” The ecological conditions that support its natural reservoir happen to be concentrated in parts of Africa. Any country connected through international travel must remain vigilant.
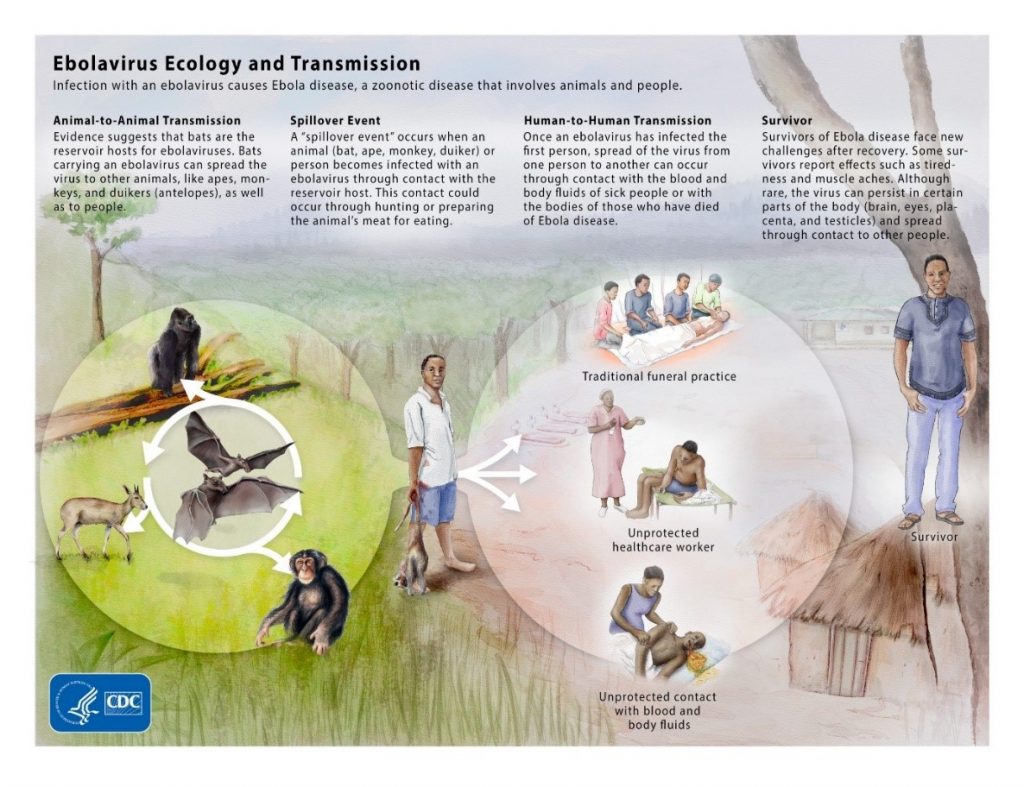
How Does Ebola Spread?
UNLIKE airborne infections such as measles or COVID-19, ebola does not spread through casual contact. Transmission occurs through direct contact with:
–Blood of an infected person.
–Vomit, stool, urine, saliva, sweat, breast milk, semen, or other body fluids.
–Contaminated needles or medical equipment.
–Bodies of deceased individuals who had ebola.
People become infectious only after symptoms develop.
Healthcare workers are particularly vulnerable if appropriate protective equipment and infection-control measures are not used. This is why strict protocols for personal protective equipment (PPE), specimen handling, environmental cleaning, and waste management are central to ebola preparedness.
Recognising the Symptoms
THE incubation period ranges from 2 to 21 days, with most patients developing symptoms within 8 to 10 days after exposure.
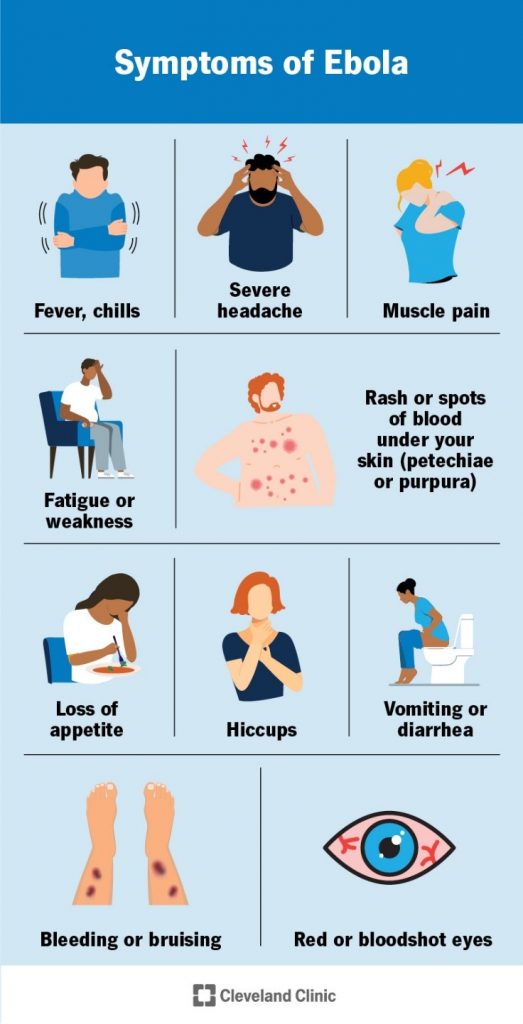
Early symptoms may resemble many common infections:
• Sudden fever
• Severe weakness
• Headache
• Muscle pain
• Sore throat
As the disease progresses, patients may develop:
• Vomiting
• Diarrhoea
• Abdominal pain
• Skin rash
• Conjunctival redness
• Liver and kidney dysfunction
In severe cases, bleeding from gums, nose, gastrointestinal tract, or injection sites may occur. Contrary to popular belief, dramatic bleeding is not present in every patient.
The challenge is that early ebola symptoms are indistinguishable from many tropical diseases. Therefore, travel history and exposure history become critically important in identifying suspected cases.
Is There a Treatment?
FOR many years, ebola was viewed as a disease with no effective treatment. Fortunately, this has changed. Early diagnosis and supportive care significantly improve survival. Treatment focuses on:
• Intravenous fluids
• Correction of electrolyte imbalance
• Oxygen support
• Blood pressure management
• Treatment of secondary infections
Monoclonal antibody therapies have shown effectiveness against certain ebola virus species and have improved outcomes when administered early. Vaccines have also transformed ebola control. The rVSV-ZEBOV vaccine has demonstrated high effectiveness against the Zaire ebola virus and has been used successfully during outbreaks to protect contacts and frontline workers.
Could Ebola Reach India?
WE must learn from lessons in Goa from SARS. In today’s interconnected world, the answer is, yes — but the risk remains low. India has substantial travel and trade links with African countries. Every year, thousands of students, professionals, business travellers, and tourists travel between India and Africa.
An imported case is therefore possible. However, imported cases do not automatically lead to outbreaks. Strong public health systems can identify, isolate, and manage cases before widespread transmission occurs. India’s experience with SARS, H1N1 influenza, Nipah virus, COVID-19, and other infectious disease threats has strengthened preparedness mechanisms considerably.
How Prepared is India?
INDIA’S preparedness strategy focuses on early detection, rapid isolation, safe laboratory testing, infection control, and coordinated public health response.
The National Institute of Virology (NIV), Pune, houses one of the country’s highest-containment laboratories capable of safely handling Ebola specimens. Hospitals have developed protocols for identifying and isolating suspected patients. Clinical specimens are transported using internationally accepted triple-packaging systems and strict biosafety standards.
Healthcare workers receive training in:
• Donning and doffing PPE.
• Safe specimen collection.
• Spill management.
• Hand hygiene.
• Environmental decontamination.
• Biomedical waste management.
• Safe ambulance transport and patient isolation.
The presentation used for hospital preparedness training highlights a critical message: “Safety of healthcare workers is important because we care.”
Travel Advisory: What Should Travellers Know?
THE World Health Organization generally does not recommend blanket travel bans during ebola outbreaks. Instead, it advocates risk-based precautions.
Travellers visiting affected regions should:
• Monitor official WHO and government advisories.
• Avoid contact with sick individuals.
• Avoid handling dead animals or bushmeat.
• Practise frequent hand hygiene.
• Avoid participation in traditional funeral rituals involving direct contact with bodies.
• Seek medical attention immediately if symptoms develop.
Anyone returning from an affected area who develops fever or other symptoms within 21 days should promptly seek medical care and disclose their travel history.
Transparency saves lives.
CONCLUSION:
The question is not whether the next outbreak will occur somewhere in the world. The question is whether we are prepared when it does. The answer must always be yes.
 LETTER TO THE EDITOR FOR ISSUE DATED JULY 25, 2026
LETTER TO THE EDITOR FOR ISSUE DATED JULY 25, 2026 NO STOPPING GEN Z NOW!
NO STOPPING GEN Z NOW! GOA STUDENTS’ ‘I AM A TERMITE’ PROTEST… GAINS ATTENTION AFTER POLITICAL REMARK!
GOA STUDENTS’ ‘I AM A TERMITE’ PROTEST… GAINS ATTENTION AFTER POLITICAL REMARK! GOAN STUDENTS RESENT BEING CALLED TERMITES!By Dr Olav & Deborah Albuquerque
GOAN STUDENTS RESENT BEING CALLED TERMITES!By Dr Olav & Deborah Albuquerque WHO SILENCED INDIA’S PROTEST STREETS?By Prabhu Chawla
WHO SILENCED INDIA’S PROTEST STREETS?By Prabhu Chawla ‘COCKROACH’ PROTESTS: MODI PROMISES TO PUNISH CORRUPT OFFICIALS IN BID TO QUELL ANGER! By Amrit Dhillon
‘COCKROACH’ PROTESTS: MODI PROMISES TO PUNISH CORRUPT OFFICIALS IN BID TO QUELL ANGER! By Amrit Dhillon WHERE IS THE MONSOON IN GOA THIS YEAR?It will be hell on earth for farmers cultivating their fields …
WHERE IS THE MONSOON IN GOA THIS YEAR?It will be hell on earth for farmers cultivating their fields … CHEAPER TO DO MBBS IN GEORGIA!
CHEAPER TO DO MBBS IN GEORGIA! INDIA’S BROKEN PROMISE How a faulty education spawned a student uprising! By Arvind Pinto
INDIA’S BROKEN PROMISE How a faulty education spawned a student uprising! By Arvind Pinto BRAIN HEALTH: ACCESS FOR ALL Rebuilding lives beyond recovery…. By Dr Vailanki Nazira Raposo
BRAIN HEALTH: ACCESS FOR ALL Rebuilding lives beyond recovery…. By Dr Vailanki Nazira Raposo OVER-ENGINEERED, UNDER-PROTECTED! The paradox of modern orthopaedic care! By Raaisa Lemos Vaz
OVER-ENGINEERED, UNDER-PROTECTED! The paradox of modern orthopaedic care! By Raaisa Lemos Vaz WORLD’S SIMPLEST PRESCRIPTION FOR A HEALTHY BRAIN!By Dr Amit Dias, MD
WORLD’S SIMPLEST PRESCRIPTION FOR A HEALTHY BRAIN!By Dr Amit Dias, MD WEEKEND UPDATESLETTER TO THE EDITOR FOR ISSUE DATED JULY 18, 2026
WEEKEND UPDATESLETTER TO THE EDITOR FOR ISSUE DATED JULY 18, 2026 THE VOICE OF PLANET EARTH… DIVING INTO ‘PRIMORDIAL’ By By Raaisa Lemos Vaz
THE VOICE OF PLANET EARTH… DIVING INTO ‘PRIMORDIAL’ By By Raaisa Lemos Vaz
Goa is abuzz with excitement as vintage bike and car owners, users, collectors and fans are decking […]